Colonoscopy is the most accurate diagnostic test for CRC. It provides direct visualization, a fairly accurate determination of the tumor location, and the opportunity to obtain tumor tissue for histologic examination. About 5% of patients will have cancerous tumors in more than one location, and the probability of additional polyps ranges from 20% to 40%. Colonoscopy provides the opportunity to remove such polyps or tattoo them so they can be removed at the time of surgery.
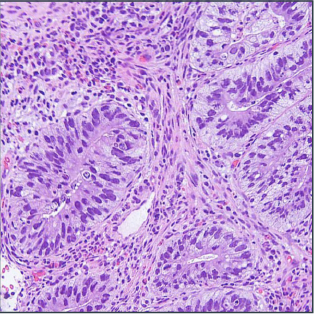
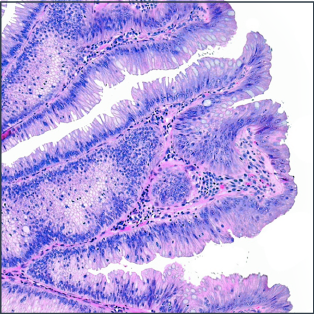
Biopsies are sent to the pathology laboratory for examination. There, the pathologist can confirm the presence of cancer and determine its type. Certain types of CRC provide information on the patient's prognosis and treatment options. Thus, some histologic phenotypes are associated with high microsatellite instability, while others are associated with a microsatellite stable genotype that has a more aggressive prognosis. Serrated adenocarcinomas are associated with BRAF mutations and MSI-H status, and have a poor prognosis.